
WHAT IS THE BEST IMPLANT POCKET FOR BREAST AUGMENTATION?
WHAT IS THE BEST IMPLANT POCKET FOR BREAST AUGMENTATION?

Breast augmentation is the most popular cosmetic procedure performed worldwide each year. It is popular due to high patient’s satisfaction with the procedure including women reporting improved body image, self-confidence, and overall sexual wellbeing. In a breast augmentation consult, I am often asked this question by my patients, “I was told by a plastic surgeon “below the muscle” is the best implant pocket for breast augmentation. Is that true?”
Foremost, choosing the tissue plane i.e. implant pocket for implant placement is one of the key factors in breast augmentation. Generally speaking, there are 3 types of implant pocket techniques in breast augmentation
- Submuscular pocket technique – Dual plane technique
- Subglandular pocket technique
- Subfascial pocket technique
A. Submuscular Pocket Technique – Dual Plane Technique
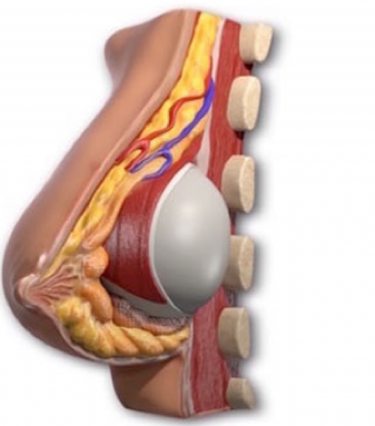
In this technique, the implant is placed behind the pectoralis major. This is accomplished by releasing the muscle origin at breast crease on the chest wall and along medial aspect of the rib cage up to the level of the fourth rib. This maneuver allows the muscle to window shade up on the chest wall as illustrated in image 1. The implant superior pole will be covered by the pectoralis major muscle and the lower pole of the implant is cover by the breast tissue, thus term dual -plane. (image 2)
Image 1.
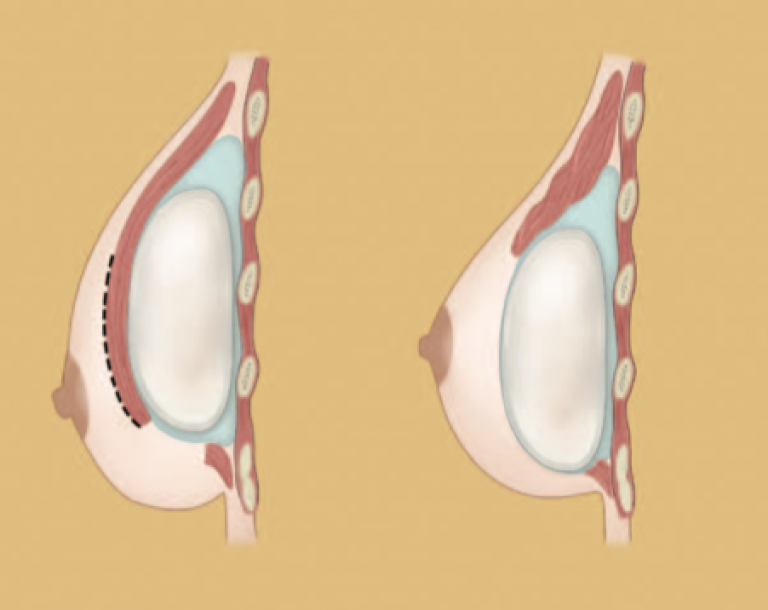
Image 2.
This technique is favored by most plastic surgeons for the following reasons:
- Increasing soft tissue coverage of the upper pole of the breasts results in less rippling and prevent shelve like appearance at the top of the breast where the implant meets the chest wall
- This technique has a reported lower rate of capsular contracture around 3 to 8
- Conceptually in the dual plane pocket, the implant sits in the subglandular pocket on the lower half of the breast which allows the implant to expand the deflated skin envelope without being limited by the pectoralis major muscle, avoiding a snoopy deformity or double bubble deformity. Snoopy deformity or double bubble deformity is characterized by breast tissue that appears to slide off the implant as appear in this picture. However, the patient in this picture had a dual plane submuscular breast augmentation
There are definite draw backs with the Dual Plane technique. Here are the main draw backs:
- There is more postoperative pain after the procedure due to the manipulation of the muscle. In some very active women with very well developed chest muscles, they do complain of long term chest discomfort and weakness.
- Animation deformity is an abnormal movement of the breast and implant due to contraction of the chest pectoralis major muscle. This is an unnatural and unnerving experiences for most women with subpectoral breast augmentation. It is not often seen in two dimensional before and after pictures. It is only evidence with movement of the arms and chest. It is most prominent in thinner patients.
- Overzealous release of the pectoralis major muscle along the sternum runs the risks of symmastia and ridge like deformity up in the chest wall.
- Submuscular dynamic laterization of the implant overtime is also a real issue that is not often listed as one of the potential draw backs of this pocket location. The contraction force of the muscle will push the implant laterally into the axilla. This is especially evident when a woman lays down and the implants will slide into the lateral chest wall.
- If the pectoralis major muscle is inadequately release, accessory muscle slips over the sternum, the implants can sits far apart resulting suboptimal cleavage. Furthermore, the implants can sit very high up in the chest wall giving a unnatural high riding implant.

Main disadvantages of Dual Plane breast augmentation
- Snoopy breast deformity or double bubble
- Wide cleave due to the limit of the pectoralis major muscle
- The technique is still prone to capsular contracture as illustrated in this patient
B. Subfascial Pocket Implant Technique
In this technique, the implant is placed below the fascia which is a layer covering the muscle. It requires meticulous dissection separating this fascial layer from the muscle. Which can be performed using a Bovie cautery in a bloodless meticulous fashion as illustrated in this picture.
- Fascia layer above the pectoralis major muscle
- Provides an additional layer to cover the implant
- Protect direct contact between the implant and breast tissue therefore lower rates of capsular contracture
- Improve cleavage in wide chest women because the location of the implant is not limited by the origin of the pectoralis muscle
- Minimal rippling even in very thin and active patient
- Most importantly No animation deformity
It is a less popular technique among plastic surgeons due to the fact that it is less frequently trained technique during residency (surgical training to become a board certified plastic surgeon). However, I personally in favor the subfascial plane over the dual plane technique for multitude of reasons
- It places the implant in a very natural plane where the added volume should be centered under the breast tissue.
- It allows the implant to expand both the breast tissue and skin in the most physiologic location where the volume should be added without the restriction of the pectoralis major muscle. This prevents any potential of double bubble or snoopy breast deformity
- No manipulation of the pectoralis major muscle, a major muscle of the chest, means less immediate postoperative pain and also discomfort in the long terms for most woman. Furthermore, it does not have the dynamic deformity force caused by contraction of the muscle or lateralization of the implant in the long term.
- Furthermore, without the limits of the muscle origin on the sternum keeping the implants apart, subfascial augmentation allows a surgeon to place the implant closer together creating a much more appealing cleavage in women with wide chest anatomy as illustrated in this patient.

5. The fascial layer provides an additional layer of coverage for the implant and prevents direct contact of between the implant and the breast parenchyma (unlike the subglandular pocket), and thus lowers the rate of capsular contracture. This has been reported in large series of subfascial breast augmentation reports in the literature. The reported rate of capsular contracture in subfascial plane is similar to that of dual plane technique.
6. For most active and athletic women, the subfascial plane allows the patient to continue with their favorite activities such as lifting weight, playing volleyball, tennis, and surfing without disrupting one of the most important chest muscles (pectoralis major muscle). These patients will not have animation deformity typical of dual plane technique.
C. Subglandular Implant Pocket Technique
In this technique, the implant is placed below the breast glandular tissue. This technique is seldomly used these days due to several factors:
- It has an abrupt sharp transition from the chest wall to the implant and thus would be less natural in appearance.
- It has potential rippling deformity due to lack of soft tissue coverage
- It has a higher rate of capsular contracture compare to the dual plane or subfascial plane
However, there are advantages to this technique
- It is less painful than submuscular or dual plane technique since there is no manipulation of the muscle
- For a deflated breast – subglandular plane does allow for expansion of the skin envelope and potentially create a lifted illusion to the breast without performing a breast lift and additional scar



